Physical therapy clinics running hybrid operations know the chaos firsthand. Morning telehealth session runs over by twelve minutes. Patient's internet cuts out mid-session, forcing a switch to phone. Meanwhile, the afternoon in-person slot needs the same provider plus specific equipment that's still being sanitized. One hiccup, and the whole day starts cascading.
Most practices treat virtual and in-person appointments like completely separate departments — different booking rules, different buffers, different equipment requirements — then scratch their heads when the hybrid scheduling falls apart after a single failure in one modality.
The problem isn't running multiple modalities. It's building operations that pretend they don't affect each other.
Why modality mixing breaks traditional scheduling logic
Traditional scheduling is built around binary checks. Provider available? Book it. Room free? Confirm it. That logic holds fine when every appointment follows the same pattern.
-
Initial video consultation (needs
provider, stable connection, HIPAA-compliant platform)
-
Follow-up in-person assessment (needs
provider, exam room, diagnostic equipment)
-
Remote monitoring check-in (needs
async provider review, data platform access)
-
Emergency phone escalation (needs
immediate provider availability, call routing)
Each modality carries different resource dependencies, different failure modes, different buffer requirements. Your scheduling system treats them as isolated events. Your operations deal with the collisions.
A dermatology practice ran into this fairly early after adding teledermatology. Their virtual appointments averaged 18 minutes, in-person averaged 24. They scheduled back-to-back, assuming the provider could handle the modality switch with minimal downtime.
What actually happened: providers needed 6-8 minutes between modalities to close virtual platforms, sanitize workstations, pull up different systems, and mentally shift gears. Those "efficient" bookings created 40-minute delays by noon. Patient satisfaction dropped from 4.6 to 3.8 stars within two months.
Buffer rules that actually prevent modality collisions
Generic buffers don't cut it for hybrid operations. You need modality-aware transition rules built around actual operational requirements.
Eliminate scheduling conflicts and missed meetings.
Schedily helps you organize and manage all appointments and team availability effortlessly.
- Unified appointment and resource management
- Automated notifications & reminders
- Team calendar synchronization
No credit card required
Same-to-same modality transitions:
-
Virtual to virtual
2-3 minute buffer (close previous session, initiate next)
-
In-person to in-person
5-7 minute buffer (room turnover, patient transition)
-
Phone to phone
1-2 minute buffer (documentation, dial next)
Cross-modality transitions:
-
Virtual to in-person
8-10 minute buffer (platform shutdown, physical prep, location change)
-
In-person to virtual
7-9 minute buffer (documentation, login to platform, tech check)
-
Emergency escalation
15-minute hold (allows proper handoff without destroying downstream schedule)
These numbers aren't arbitrary. A mental health practice tracking roughly 2,400 appointments found that enforcing 10-minute buffers between modality switches reduced delays by 67% while pulling back daily capacity by only about 4%.
Track actual transition time by provider for each modality pair and update buffers quarterly to reflect real workflows.
The tradeoff is obvious once you see it. Slightly longer buffers cost far less than cascading delays from inadequate transition time.
Equipment availability modeling across modalities
Equipment conflicts in hybrid operations tend to sneak up on you. The ultrasound machine sits unused during morning telehealth blocks. High-resolution cameras for virtual dermatology exams get borrowed for in-person documentation. Nobody tracks cross-modality equipment dependencies until something actually breaks down.
Smart availability modeling means mapping equipment to both primary and secondary modality uses:
| Equipment Type | Primary Modality | Secondary Uses | Conflict Zones |
|---|---|---|---|
| Diagnostic tablets | In-person exams | Virtual show-and-tell | Morning overlap periods |
| Specialized cameras | Telehealth | In-person documentation | Midday transitions |
| Monitoring devices | Remote patient monitoring | In-person spot-checks | Emergency escalations |
| Exam room screens | In-person consultations | Virtual second opinions | Hybrid appointments |
A cardiology practice ran into this after their remote monitoring program expanded. Holter monitors worked well for 48-hour remote recordings — but were also needed for immediate in-office EKGs. Nobody mapped the overlap until emergency appointments couldn't access equipment "reserved" for remote patients who wouldn't return devices for days.
The fix wasn't buying more hardware. It was creating modality-aware equipment pools with clear checkout rules. Remote monitoring got dedicated units. Emergency equipment stayed protected. Shared resources got booking priorities based on modality type and urgency. Equipment conflicts dropped from around twelve per week to two.
Escalation paths when modality segments fail
Virtual appointment fails? Default response is to reschedule. Except when that virtual appointment was segment one of a three-part hybrid journey. Now you've got downstream dependencies, equipment holds, and potentially urgent care needs sitting in limbo.
Virtual segment failures:
-
Technical failure → Immediate phone backup (same slot)
-
Provider no-show → Async message + priority reschedule
-
Patient no-show → Automated recovery flow + in-person option
In-person segment failures:
-
Equipment unavailable → Virtual alternative assessment
-
Room conflicts → Overflow to telehealth room
-
Provider emergency → Remote provider covers history and documentation
Hybrid appointment chains:
-
Early segment fails → Hold downstream resources for 30 minutes
-
Mid-chain failure → Preserve completed segments, reschedule remaining
-
Final segment fails → Mark partial completion, trigger follow-up
An orthopedic surgery practice built these paths after losing around $12,000 in one month from broken appointment chains. Patient completes virtual pre-op consultation. In-person imaging fails due to equipment issues. Surgery gets cancelled. Insurance refuses payment for an incomplete assessment pathway.
Their new escalation logic: any chain failure triggers immediate clinical review. Provider determines whether remaining segments can proceed independently. System holds all downstream resources for 48 hours while resolution plays out. Completion rate for multi-segment journeys climbed from 62% to 84%.
Cross-modality SLA mapping
Your telehealth platform promises 2-minute connection times. In-person operations target 10-minute wait times. Phone system guarantees 30-second pickup. These SLAs exist in isolation with no accounting for how modality transitions affect total service delivery.
Real SLA mapping covers the full patient journey across modalities. A patient starting with a virtual consultation expects consistent service when transitioning to in-person follow-up. Breaking SLA in one modality colors how they experience your entire practice.
Response time stacking:
-
Initial contact SLA
5 minutes (any modality)
-
Modality transition SLA
15 minutes maximum
-
Total journey SLA
90 minutes for urgent, 4 hours for routine
Handoff requirements:
-
Context must transfer between modalities (no repeated intake)
-
Previous modality data visible in next segment
-
Provider notes accessible across platforms
Failure recovery:
-
If one modality breaks SLA, next modality gets priority handling
-
Cumulative delay triggers automatic escalation
-
Journey SLA overrides individual modality targets
A multi-specialty clinic group mapped these after patients kept complaining about "starting over" at each appointment type. Despite meeting individual modality SLAs, total patient journey times averaged 5.5 hours for complex cases. Cross-modality coordination brought that to 2.5 hours without touching individual appointment lengths.
Building operational resilience into mixed-modality scheduling
This workflow visualizes modality transitions, buffer checkpoints, equipment holds, and escalation decision points across a multi-segment patient journey.
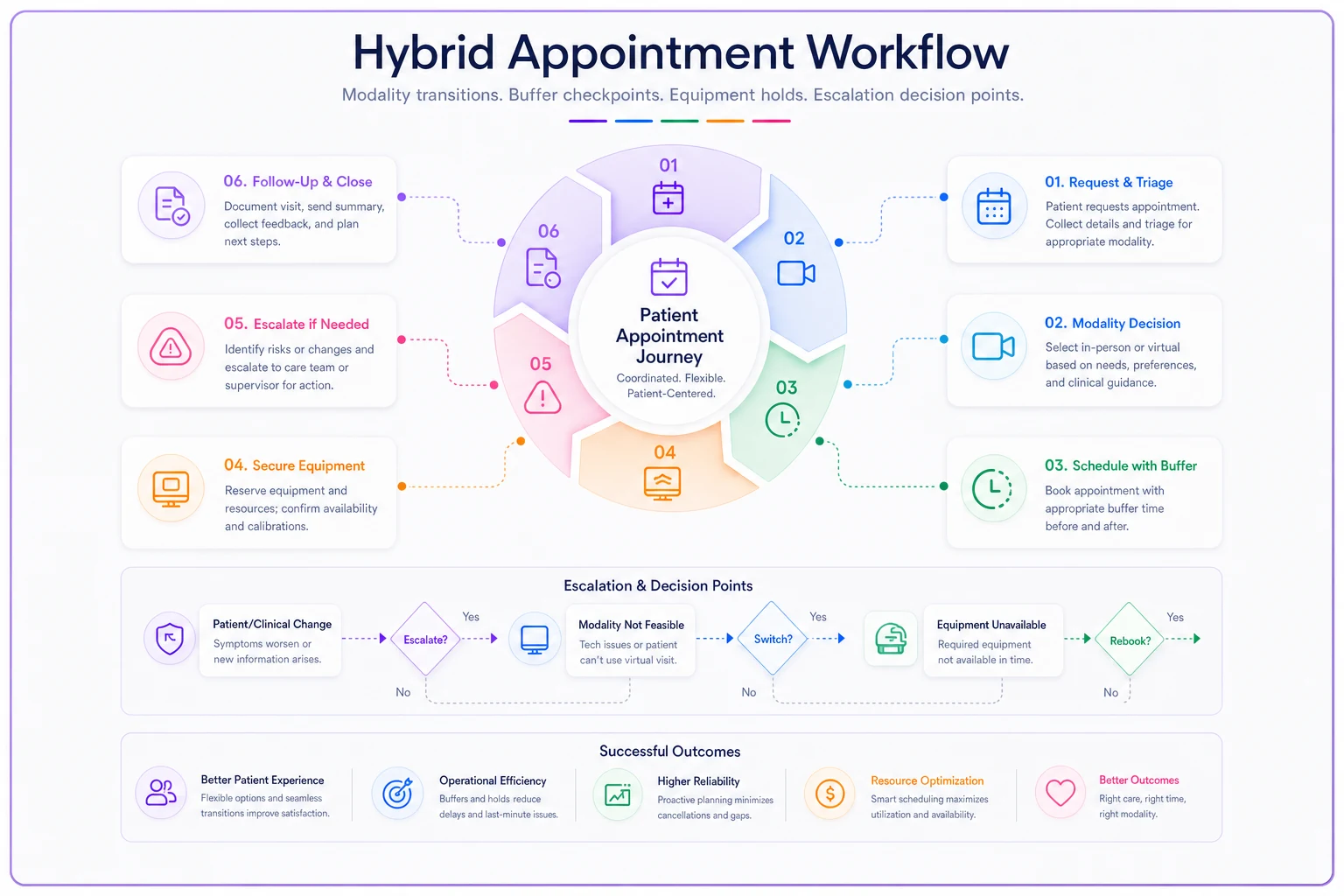
Practices that run hybrid appointment scheduling well don't just accommodate multiple modalities — they build operations where modality mixing is the default assumption, not an edge case.
-
Equipment can serve multiple modalities but needs transition time between them
-
Providers need different prep depending on modality type
-
Patients judge service across the full journey, not individual touchpoints
-
Failed segments in appointment chains need immediate decision logic, not manual intervention
-
Buffer times prevent more problems than they cause
A primary care network running around 14,000 monthly appointments across three modalities figured this out through some painful trial and error. Their first attempt treated virtual as "regular appointments but online." Didn't work. Second attempt gave virtual its own separate schedule — also a mess, because providers kept switching contexts without proper transitions.
Third approach: unified scheduling with modality-aware logic built in. The system knows Dr. Patterson needs 8 minutes between virtual and in-person because she changes into scrubs. Exam room 3's camera setup makes it the best fit for hybrid appointments. Thursdays run heavy telehealth mornings, so equipment gets staged differently the night before.
Result: 23% reduction in delays, 31% improvement in provider satisfaction, roughly $47,000 monthly recovery from previously lost appointment slots — not from adding capacity, but from understanding that hybrid operations need hybrid operational logic.
The operational reality of mixed-modality practices
Running hybrid appointment scheduling isn't really about choosing between virtual and in-person anymore. It's about coordinating complex resource dependencies across multiple delivery channels while keeping service quality intact.
Practices that do this well don't rely on providers to manually juggle modalities. They build operational intelligence into their scheduling systems. Smart resource coordination becomes especially important when you're managing equipment, rooms, and providers across different modality requirements at the same time.
AI-powered operational software can track these dependencies automatically — adjusting buffers based on historical patterns, flagging equipment conflicts before they surface on the schedule, routing failures to the right escalation paths without someone manually intervening every single time.
The math isn't hard. A practice running 400+ hybrid appointments monthly can easily lose 12-15% of capacity to modality transition friction. That's 48-60 appointments. At $125 average reimbursement, you're looking at $6,000-$7,500 left on the table every month from scheduling inefficiency alone.
But the revenue loss is almost secondary to what it actually costs operationally. Provider burnout from constant context switching. Patient frustration from broken appointment chains. Staff exhaustion from manually coordinating across systems that were never designed to talk to each other. Fix the modality transition logic. Map the equipment dependencies. Build escalation paths that function when something breaks. Stop treating virtual and in-person appointments like they exist in separate operational worlds — because your providers, your equipment, and your patients definitely don't.
Ready to optimize your scheduling and operations?
Join thousands of businesses using Schedily to save time, improve coordination, and enhance operational efficiency.